
SLIDE 1
10/10/2017 1
Screening, evaluation and treatment of dementia in the elderly Asian population
Aimee Kao, MD, PhD Associate Professor of Neurology UCSF Asian Health Symposium 2017.10.05
No disclosures
Outline of talk
- Introduction
- Dementia definition and syndromes
- Case study
- Special issues in the Asian community
- UCSF Chinese Outreach Clinics
Why is dementia important?
- Rapidly aging population
- Alzheimer Disease is the 6th leading
cause of death in the U.S.
- 5.4 million individuals affected
- 1 in 8 Americans aged 65 and older is affected by
Alzheimer’s Disease
- In 2013, Americans provided provided 17.7 billion
hours of unpaid care to people with AD and other dementias
- In 2014, AD cost Medicare and Medicaid ~$150 billion
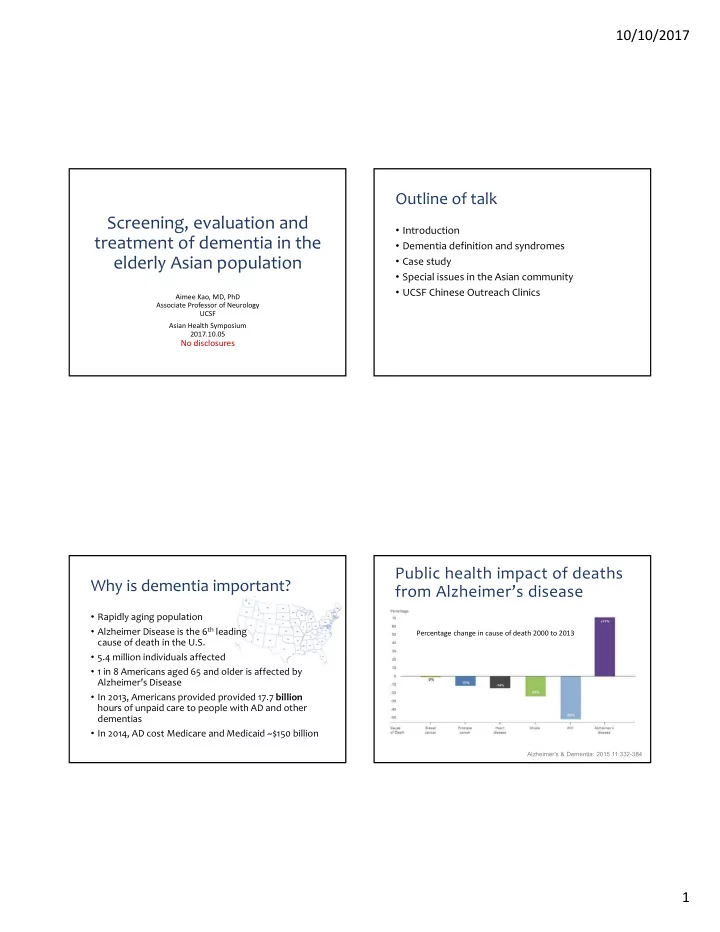
Alzheimer's & Dementia: 2015 11:332-384
Percentage change in cause of death 2000 to 2013