
PEPtalkTM Weight Management: Talking to Your Overweight Patients About Weight Loss Therapies 1
PEPtalkTM Weight Management: Talking to Your Overweight Patients About Weight Loss Therapies
Primary Care Decision-Making for Success
Scott Kahan, MD, MPH, FTOS Director, National Center for Weight and Wellness Clinical Director, Strategies to Overcome and Prevent (STOP) Obesity Alliance George Washington University Milken Institute of Public Health Washington, DC Paul P. Doghramji, MD, FAAFP Family Physician Collegeville Family Practice Medical Director of Health Services Ursinus College Collegeville, PA
Best Practices Pearls
Evaluate and Measure: Body Mass Index (BMI) Waist circumference Metabolic risk factors Discuss Risk and health benefits of 5%-10% weight loss Counsel Lifestyle or refer to a lifestyle modification Propose Medication Adjuncts appropriately Decide on Best Therapy to achieve weight loss goals Evaluate Efficacy: Modify therapy to achieve success
Body Weight
Pressures to Eat More Pressures to Be Less Physically Active
Biology Behavior
Ein Eout
Portion Sizes Soft drinks/junk food Variety High Energy density in schools Convenience High glycemic index Added Sugar Great Taste Low Cost Easy food access Ads/marketing Sedentary workplaces/schools/ entertainment Activity “unfriendly” community design Drive-through conveniences Elevators/escalators Remote controls Labor-saving devices Television/computer 0.0 0.5 1.0 1.5 2.0 2.5
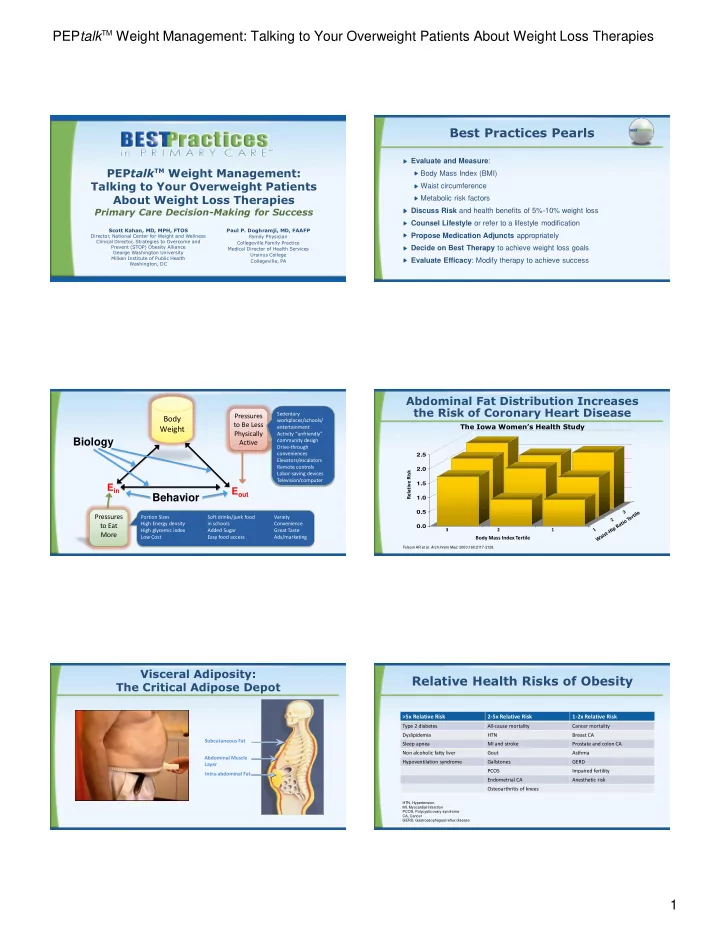
Folsom AR et al. Arch Intern Med. 2000;160:2117-2128.
Body Mass Index Tertile 3 2 1 Relative Risk
Abdominal Fat Distribution Increases the Risk of Coronary Heart Disease
The Iowa Women’s Health Study
Subcutaneous Fat Abdominal Muscle Layer Intra-abdominal Fat
Visceral Adiposity: The Critical Adipose Depot
Relative Health Risks of Obesity
>5x Relative Risk 2-5x Relative Risk 1-2x Relative Risk Type 2 diabetes All-cause mortality Cancer mortality Dyslipidemia HTN Breast CA Sleep apnea MI and stroke Prostate and colon CA Non alcoholic fatty liver Gout Asthma Hypoventilation syndrome Gallstones GERD PCOS Impaired fertility Endometrial CA Anesthetic risk Osteoarthritis of knees
HTN, Hypertension MI, Myocardial Infarction PCOS, Polycystic ovary syndrome CA, Cancer GERD, Gastroesophageal reflux disease