
SLIDE 1
10/20/2017 1
Across the Lifespan with PCOS and Reproductive Care: A focus on adolescents, fertility and aging
Heather Huddleston, M.D. Associate Professor Director of UCSF Multidisciplinary Clinic for Women with PCOS
University of California, San Francisco
Outline
- Diagnostic Criteria and PCOS features
- Diagnostic Criteria by age
- Care for the woman with PCOS, with a focus on:
– Adolescence – Fertility and pregnancy – Post Reproductive
PCOS Criteria Phenotypes
Hyperandrogenism Oligo or Anovulation Polycystic Ovaries Other Features:
- Insulin Resistance
- Obesity
- Metabolic Syndrome
- Depression
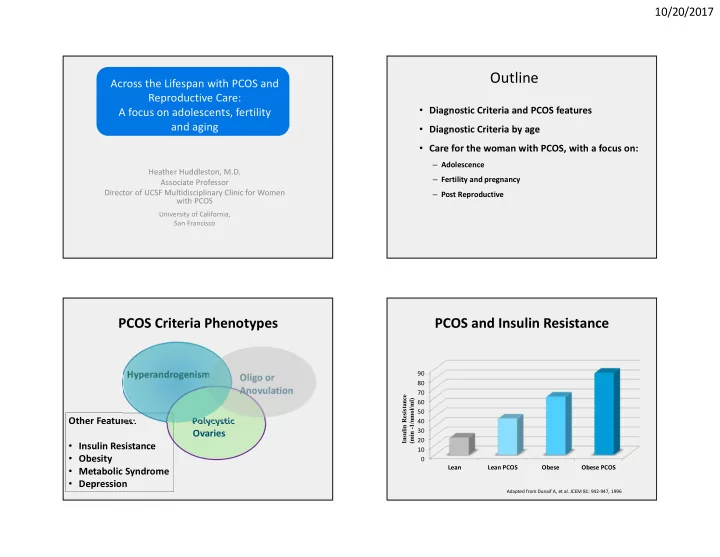
PCOS and Insulin Resistance
10 20 30 40 50 60 70 80 90 Lean Lean PCOS Obese Obese PCOS Insulin Resistance (min -1/nmol/ml)
Adapted from Dunaif A, et al. JCEM 81: 942-947, 1996