
2/25/2019 1
Choosing the Right Treatment Regimen
Hemant Shah MD MScCH HPTE Jordan Feld MD MPH
What is the role of primary care in HCV management?
- 1. Diagnosis – screening
- 2. Staging of disease
- 3. Preventing progression
- 4. Treatment!
- 5. Follow-up after treatment
Access to Treatment
- Access for all!
- No fibrosis restrictions
- Limited provider restrictions
- No sobriety restrictions
- All patients with chronic HCV are eligible for treatment
- Limited use codes – very easy!!
- HCV RNA positive x 2 more than 6 m apart (exclude spontaneous clearance)
- GI, ID or “provider experienced in HCV treatment”
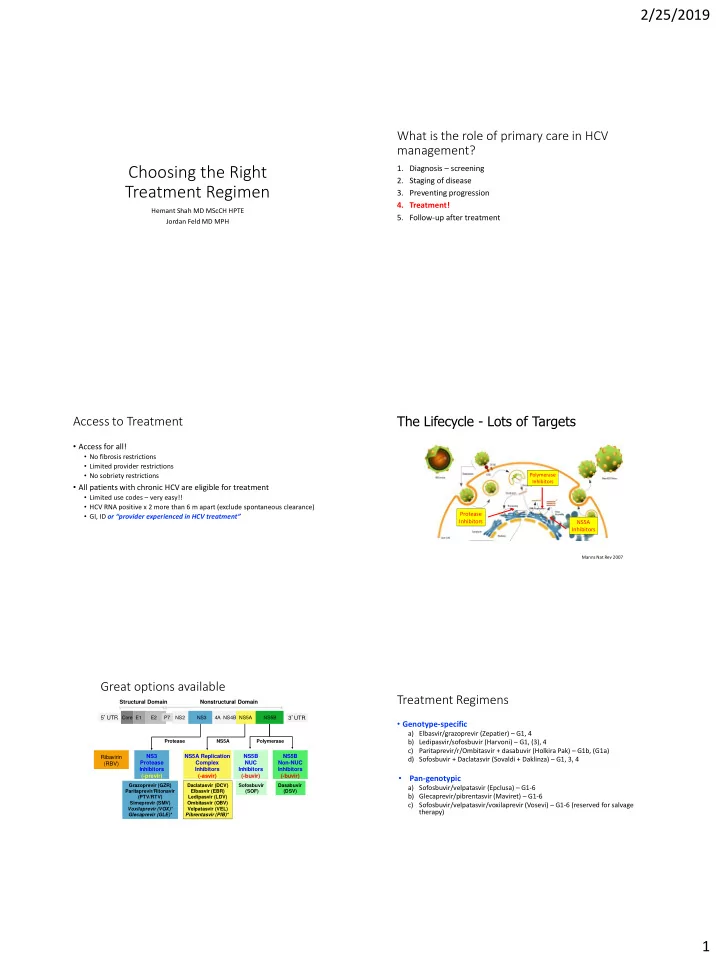
The Lifecycle - Lots of Targets
Manns Nat Rev 2007
Protease Inhibitors Polymerase Inhibitors NS5A Inhibitors
Great options available
3’UTR 5’UTR Core E1 E2 NS2 NS3 NS5A NS5B P7 Ribavirin (RBV) Polymerase Daclatasvir (DCV) Elbasvir (EBR) Ledipasvir (LDV) Ombitasvir (OBV) Velpatasvir (VEL) Pibrentasvir (PIB)* Sofosbuvir (SOF) Dasabuvir (DSV) NS5B NUC Inhibitors (-buvir) NS5A Replication Complex Inhibitors (-asvir) NS5B Non-NUC Inhibitors (-buvir) Grazoprevir (GZR) Paritaprevir/Ritonavir (PTV/RTV) Simeprevir (SMV) Voxilaprevir (VOX)* Glecaprevir (GLE)* NS3 Protease Inhibitors (-previr) Protease Structural Domain 4A NS4B Nonstructural Domain NS5A
Treatment Regimens
- Genotype-specific
a) Elbasvir/grazoprevir (Zepatier) – G1, 4 b) Ledipasvir/sofosbuvir (Harvoni) – G1, (3), 4 c) Paritaprevir/r/Ombitasvir + dasabuvir (Holkira Pak) – G1b, (G1a) d) Sofosbuvir + Daclatasvir (Sovaldi + Daklinza) – G1, 3, 4
- Pan-genotypic
a) Sofosbuvir/velpatasvir (Epclusa) – G1-6 b) Glecaprevir/pibrentasvir (Maviret) – G1-6 c) Sofosbuvir/velpatasvir/voxilaprevir (Vosevi) – G1-6 (reserved for salvage therapy)