
SLIDE 1
ASDIN 7th Annual Scientific Meeting 1
Percutaneous Salvage of Thrombosed I A F l
Gregg A. Miller MD Gregg A. Miller MD Assistant Clinical Professor, Columbia P & S Assistant Clinical Professor, Columbia P & S Chief Medical Officer, American Access Care Chief Medical Officer, American Access Care
Immature Arteriovenous Fistulas Based on 2007 ESRD Medicare data
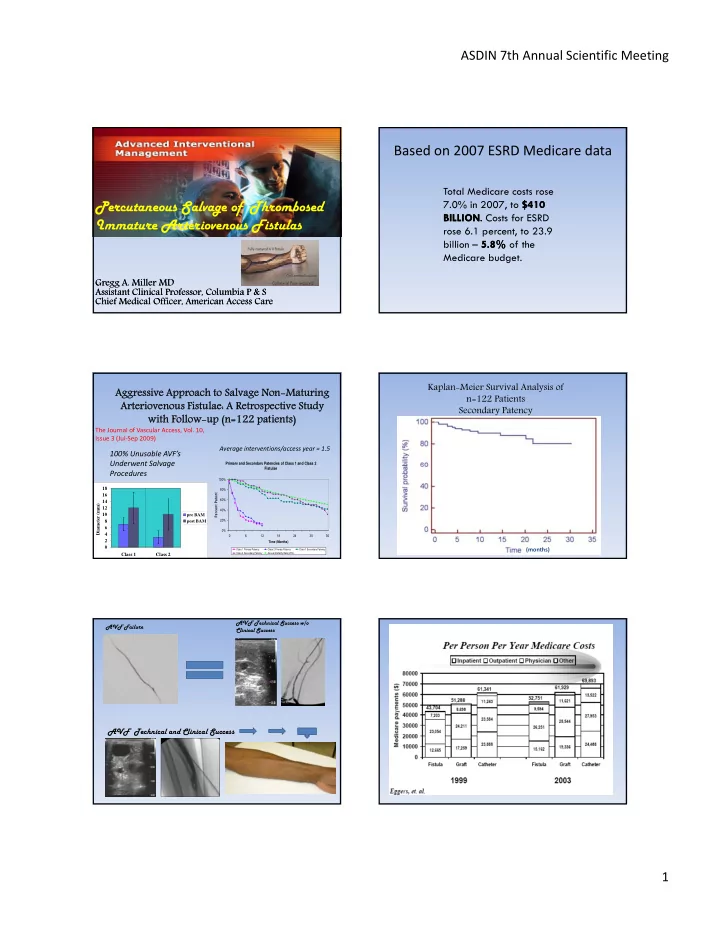
Total Medicare costs rose 7.0% in 2007, to $410 $410 BILLION BILLION. . Costs for ESRD BILLION BILLION. . Costs for ESRD rose 6.1 percent, to 23.9 billion – 5.8% 5.8% of the Medicare budget. Aggres Aggressiv sive Approach Approach to to Salvage Salvage Non-Maturing Non-Maturing Arteriovenous Arteriovenous Fistulae: A istulae: A Retrospect Retrospective Study ive Study with Follow-up with Follow-up (n=122 patients) (n=122 patients)
The Journal of Vascular Access, Vol. 10, Issue 3 (Jul‐Sep 2009)
Primary and Secondary Patencies of Class 1 and Class 2
100% Unusable AVF’s Underwent Salvage
Average interventions/access year = 1.5
2 4 6 8 10 12 14 16 18 Class 1 Class 2 Diameter (mm) pre BAM post BAM
Fistulae 0% 20% 40% 60% 80% 100% 6 12 18 24 30 36 Time (Months) Percent Patent
Class 1 Primary Patency Class 2 Primary Patency Class 1 Secondary Patency Class 2 Secondary Patency Annual Mortality Rate (20%)
Underwent Salvage Procedures
Kaplan-Meier Survival Analysis of n=122 Patients Secondary Patency
(months) AVF Failure AVF Technical Success w/o Clinical Success