
8/5/2013 1
OUTPATIENT MANAGEMENT OF CAD- A PRIMARY CARE PERSPECTIVE
Michael G. Shlipak, MD, MPH Professor of Medicine, Biostatistics, and Epidemiology Chief, General Internal Medicine August 5, 2013
FEATURES OF THIS TALK
It’s a debut Covers a broad array of topics Greatest attention to common challenges in decision
making
All recommendations supported by the following
Guideline: AHA Guideline for the Diagnosis and Management of Patients with Stable Ischemic Heart Disease (Circulation, 2012)
Class 1 indication: we should do this Class 2 indication: it’s reasonable to do this
QUESTION #1
YOUR PATIENT IS A 62YO MAN WITH HISTORY OF CONTROLLED HYPERTENSION, MILD OVERWEIGHT (BMI 29), AND UNTREATED LDL OF 137MG/DL. HE REPORTS TO YOU THAT FOR ABOUT 2 MONTHS HE HAS EXPERIENCED LEFT-SIDED CHEST TIGHTNESS AFTER WORKING UP 2 FLIGHTS OF STAIRS . IT IS RELIEVED BY REST AND IS NOT PROGRESSING NOTICEABLY. THE SYMPTOMS HAVE NOT OCCURRED AT ANY OTHER TIMES. WHAT IS THE PROBABILITY THAT THE PATIENT’S SYMPTOMS ARE CAUSED BY CAD?
< 5 % 6 % 8 % > 9 %
10% 52% 25% 13%
a)
<50%
b)
60%
c)
80%
d)
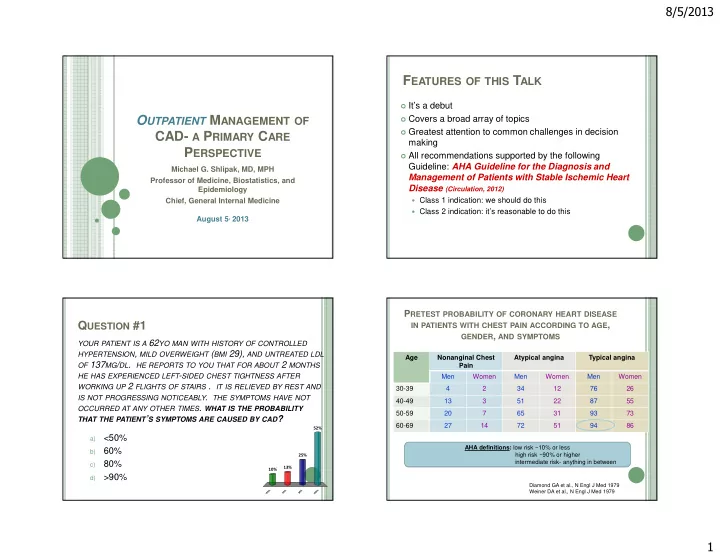
>90% PRETEST PROBABILITY OF CORONARY HEART DISEASE
IN PATIENTS WITH CHEST PAIN ACCORDING TO AGE, GENDER, AND SYMPTOMS
Age Nonanginal Chest Pain Atypical angina Typical angina Men Women Men Women Men Women 30-39 4 2 34 12 76 26 40-49 13 3 51 22 87 55 50-59 20 7 65 31 93 73 60-69 27 14 72 51 94 86
Diamond GA et al., N Engl J Med 1979 Weiner DA et al., N Engl J Med 1979
AHA definitions: low risk ~10% or less high risk ~90% or higher intermediate risk- anything in between